“We cannot solve our problems with the same thinking we used when we created them”
Albert Einstein
The current standoff (2026) between Prince Edward Island family physicians and Health PEI is likely reflective of a larger trend in medicine, and healthcare in general: dehumanization.
The doctors want the opportunity to provide humane person-centred care, with empathy and emotional presence … while also guarding their own humanity from moral injury, family neglect, and unwellness. These two poles are being driven apart in PEI (and much of Canada) by pressures from bureaucrats to address the legitimate primary care needs of the public. In our Canadian context, that means spending healthcare tax dollars effectively and efficiently. But in that pressure, doctors report feeling disrespected and stripped of their autonomy and agency, less than human—dehumanized.
Meanwhile patients, unable to reach a human voice at their doctor’s office, or losing their family doctor, or awaiting a callback from 811, or sitting in an ER for hours, feel devalued and uncared for. Also dehumanized.
Dehumanizing Healthcare
The dehumanization of medicine and healthcare in both Canada and the US has become an increasingly discussed concern among patients, clinicians, and policymakers alike. While both our countries have highly advanced medical systems capable of remarkable technological and scientific achievements, many argue that the human dimension of care—empathy, relationship, and individualized attention—has been steadily eroded.
The ongoing current crisis here on PEI (a fourth family doctor just announced practise closure) should pause us all for some deeper, even existential, reflection. Even before the Covid-19 pandemic, researchers and ethicists were starting to explore the effects of dehumanized and institutionalized healthcare on both patients and providers.
The cost dehumanization and lack of trust
In my CBC interview with Mitch Cormier, the subsequent news article, and in my written post, I reflected on what I see as 5 reasons for family doctors’ excessive administrative load. I thought of it as a “30,000 feet view.” Now, in this piece I reflect with even a wider and higher view.
The labour dispute that became very public is very indicative of what Stephen M.R. Covey (Jr) in his book The Speed of Trust, calls a low trust tax. (You can find an overview of his book and work here). Basically, the lower the trust in an organization, the higher the “tax” inconspicuously being levied (costing time, labour, and productivity).
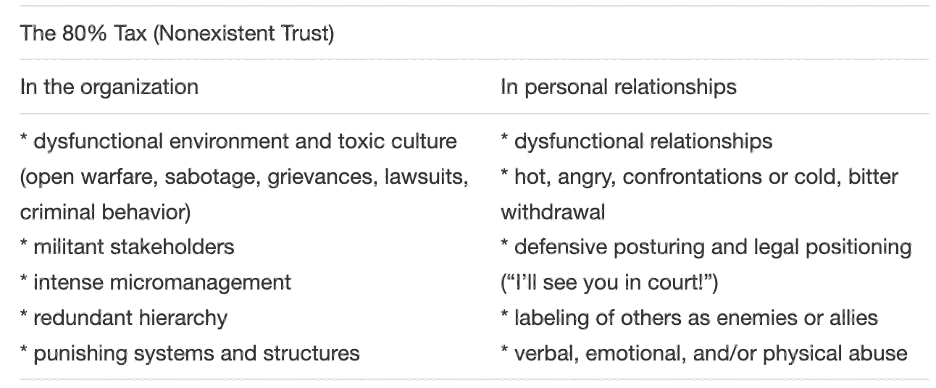
Unfortunately, using Covey’s diagnostic criteria in Figure 1, right now, our PEI health system is suffering from an 80% tax (which makes sense given the backlog, the waits, the unprofessional behaviour, lawsuit threats).
High trust organizations have an opposite “tax” – a “dividend,” as in the figure below:
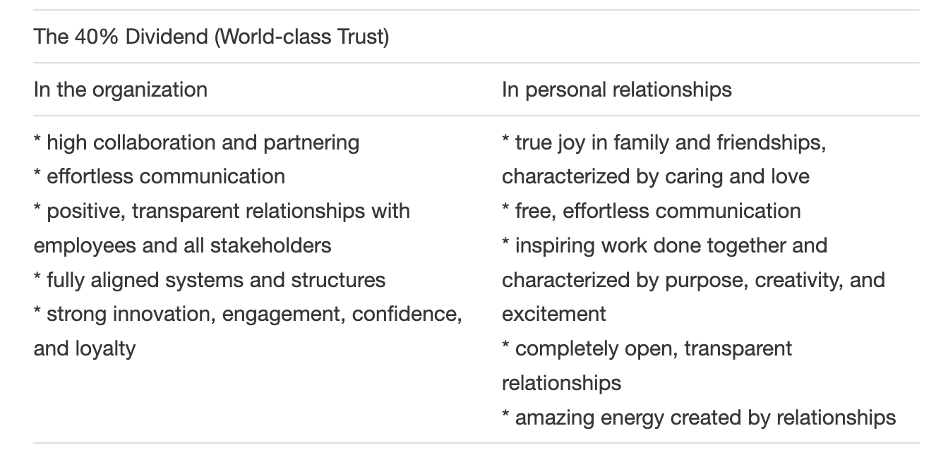
Why oh why, can we not, in this tiny province achieve that? As Mahatma Gandhi said, “The difference between what we are doing and what we’re capable of doing would solve most of the world’s problems.”
How do we rehumanize healthcare?
Impressed by an incredible local restaurant that in my opinion has the best food and service on PEI, I asked the owner what her secret to success was. She answered with one word: “Love.”
Love your people, and your customers.
Simon Sinek famously puts it this way: “Leadership is not about being in charge. Leadership is about taking care of those in your charge“
Or Jim Collins, author of Good to Great: “True leadership is the art of getting people to want to do what must be done.”
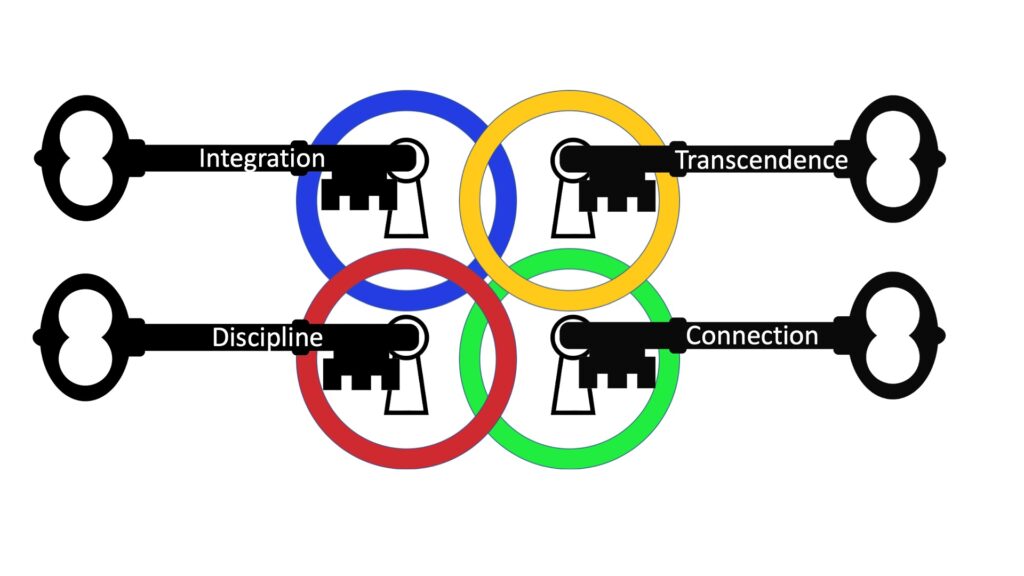
I am going to suggest 4 Keys to Sustainable Compassionate Healthcare based on the four human intelligences that I learned from the late Stephen R Covey (Sr) in The 8th Habit (his leadership sequel to his world famous 7 Habits of Highly Effective People). All four keys MUST be applied to unlock the fortress we build around ourselves and our institutions. They are individual keys for our own growth and healing from the inevitable brokenness and traumas we bring to our workplaces, and these keys are writ large for governments, organizations, faith communities, and families.
Here is a brief overview in the Table below:
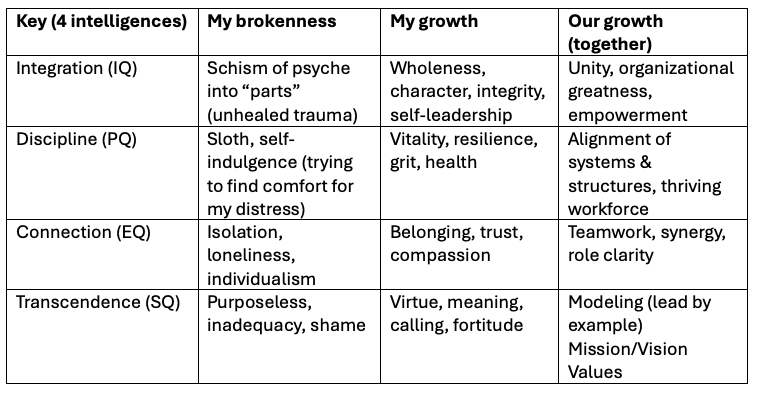
I will be expanding on each key in subsequent posts. The first one, Integration, may not be obvious to readers unfamiliar with the now gold standard of being “trauma informed.” A good introduction to this is the work by Dr. Richard Schwartz in the Internal Family Systems (IFS) model (see his book, No Bad Parts).
In order to reach Covey’s 40% dividend (world class trust), all of us as stakeholders need to begin our own “My Growth” journey. Then we can achieve “Our Growth,” achieve peace between the current warring parties, and begin to achieve better health and healthcare for ALL Islanders.
Respectfully and humbly submitted,
Hendrik Visser, MD
For my detailed Discussion Paper on Dehumanization of Medicine and Healthcare, download a PDF copy here. The first two pages are an Executive Summary. Suggested further reading and peer reviewed research papers on Dehumanization are referenced.