Dr. Jane Philpott, former federal Minister of Health and current Dean of the Faculty of Health Sciences at Queen University, has written a beautiful book which every healthcare and political leader in Canada should read (in my opinion, regardless of political stripe). Both as a memoir of her medical career beginning in Africa and an early adopter of the “Medical Home” vision for family medicine, and a detailed template for universal primary care for every Canadian, she calls for a new “Canada Primary Care Act.”
She writes,
“The transition to universal primary care will happen faster if there is a shared vision with loud public demand for and expectation of such a system. We will not be successful unless clinicians are on board. Most of all, we will need the unrelenting determination of political leaders in all orders of government, of all stripes, who will fight for this vision on behalf of Canadians and not stop until it is accomplished.”
Health for All: A Doctor’s Prescription for a Healthier Canada by Jane Philpott https://a.co/21IOl3H
She goes on to compare primary care to education in Canada–every child is expected to have access to publically funded education. She says Canadians should expect the same with access to primary care within 30 minutes of their home. And she says this can be accomplished if there is the will of leaders.
I admire Jane’s forthright writing about her journey as a caring physician for her patients and global health. And her days as a politician.
There is much handwringing and finger pointing regarding the state of Primary Healthcare in Canada. If not daily, certainly weekly, media reports highlight the shortage of family physicians. And deaths from virtual care misdiagnoses. Groups such as our own Retired Physicians Advocacy Group are writing and posting reports with suggested solutions.
Here is a recent one, Primary Care Needs Our Care, available on the OurCare.ca website, principally authored by Dr. Tara Kiran, a family physician from St. Michael’s in Toronto. This included a national survey and several provincial “Priorities Panels,” essentially multidisciplinary round tables. Their key themes and recommendations are identified on page 7.
I would recommend a close reading of this excellent work by our political and healthcare leaders.
The angle of more spending on prevention and the determinants of health was emphasized by another group called Generation Squeeze. Their report, Health is More Than Medical Care, is authored by Paul Kershaw, Ph.D, UBC School of Population and Public Health. Their website is GetWellCanada.Ca . The CBC recently highlighted this work, reporting that the authors “call for better funding of housing, child care and education to improve population health.”
In this post I will add some additional reflections on how I believe we got where we are. The corollary is of course that by identifying these factors, we could potentially reverse these barriers in the long term.
I will highlight what I believe to be four contributing factors:
Primary care in Canada has entered a “grey zone” – a liminal state
“Everything rises and falls on leadership” – and on followership
The workforce (and society) have become “fragile” – not only a lack of resilience
Mainstream western medicine continues entrenched on the Cartesian foundation of dualism
Primary care has entered a grey zone
The space between the end of an era and the faltering or sputtering new era is sometimes referred to as a “grey zone.” Or a liminal state. The leader’s vision for the new era may be foggy and there may not be unity or buy in by all followers. Policies and procedures are likely being tested as drafts. So, the new era may lead to polarization, conflict, and poor performance.
The “golden era” of family medicine began in Canada under Medicare in the early 60’s and had a quite abrupt end in the 1990s when Canadian political leaders decided to address rising healthcare costs by rationing access. For those with a memory of those days, Dr. Marcus Welby was the ‘poster boy’ of this era. Everyone had their own caring, kind, family doctor. They were generally self-led, owner operators of their own small (or larger clinics) domain. They got paid for their work, although often poorly compared to other similar professionals. They hired their own staff. Through volume and large practises, they (I included) made a decent living.
The new era of family medicine is marked by the “Medical Home” concept, interdisciplinary teams under one roof. Globally, this is not a new idea. Personally, I entered the profession in West Africa in 1980 under this model, and together with non-physician primary health care workers, nurses, and midwives, we (around 8 to 10 MDs) largely looked after a population of around 2 million people.
But here in Canada, and on PEI, we have not yet “hit our stride,” under this new model. Where promises were made that this new way would quickly eliminate the “patient registry” of individuals and families without a family doctor or nurse practitioner, this has not yet happened. Negotiations here (and in other provinces) are underway to appropriately remunerate family physicians under the new model. We are all hopeful that this will attract more young physician graduates into a family medicine career.
But meanwhile, here is what is missing, in my opinion—synergistic teamwork. Medical homes can only be high performing when the sum of the individual contributions is greater than those individuals working on their own (or in other facilities). That’s the definition of synergy: 1 + 1 > 2.
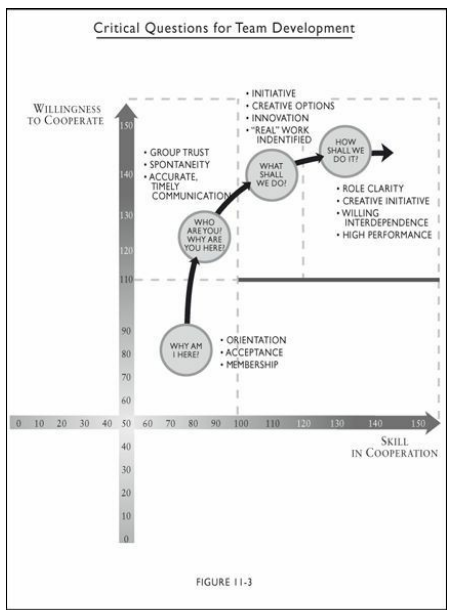
In his book, The Performance Factor, author Pat MacMillan has illustrated what is required for a team to be high performing and which questions must be addressed (Both Skill in Cooperation and Willingness to Cooperate are needed – see figure below):
Image Credit: MacMillan, Pat. The Performance Factor: Unlocking the Secrets of Teamwork . B&H Publishing. Kindle Edition.
He writes,
“Largely through ignorance, many teams never address these questions and spend most of their time drifting through a fog of ineffectiveness characterized by defensiveness, mistrust, game-playing, and politics, apathy, competition, and conflict.”
Pat MacMillan, Location 3640
The willing interdependence needed is quite countercultural to our current societal trend toward hyper-individualism. I am however, hopeful that our PEI Medical homes are becoming high performing teams and much rests on how they are being led—their team leader.
Leadership and followership
According to leadership expert and prolific writer, John C. Maxwell, “Everything rises and falls on leadership.” Family physicians were traditionally self-led and intrinsically motivated. And in the historical hierarchal command and control healthcare industry, physicians were over nurses, and so on down the line. In this new era, the leadership dynamics are changing, and many managers are nurses or business graduates.
Many family physicians are now opting to be led. So, they need to be followers. To quote MacMillan again, they need to be “rowing in the same direction.” This means a shared passion for the mission and vision of the organization. A social contract marked by civic responsibility for the greater community good, rather than one’s own self-centered needs (a healthy interdependence) is what I believe is needed.
Robert Bly was already warning readers of the trend toward individualism back in 1996 in The Sibling Society:
“We all recognize that our emphasis on individualism in the West has dimmed whatever instincts Western youth might have had to preserve the troop. For some time now our own spark of life has been more compelling, more important to us, than the flame of the larger group.”
Robert Bly, The Sibling Society
Many employees in the healthcare industry (and the workforce in general), including physicians, have also been influenced by the so-called “slow productivity movement,” highlighted by media reports of “quiet quitting” and “the great resignation.” The Covid-19 pandemic certainly encouraged these trends. Certainly, this trend is not all bad. Workism (work as god), and workaholism (an addiction), both damage individuals and families. Cal Newport has written a fascinating book on this, Slow Productivity: The Lost Art of Accomplishment Without Burnout. He highlights 3 ways: 1) Do fewer things 2) Work at a natural pace and 3) Obsess over quality.
High performing Medical Homes without chaos and unnecessary hurry or working late are possible. It requires great role clarity, efficient phone service (or on-line equivalent), great triaging, and a system of saving space for same day (in-person) urgent cases. And the efficient use of IT. Our Retired Physicians Advocacy Group has written a draft potential workflow template.
But there will be times when we will need to do hard things (like during a pandemic, or a natural disaster). How we learn to handle the winds of adversity are a key to high performing teams and personal well-being and resilience (by becoming antifragile).
Cultural fragility
A lot has been spoken and written recently about resilience, the ability to bounce back to baseline after something hard. Family medicine is hard. I know. I was there for 32 years looking after over 2000 people. It takes commitment and dare I say, “love” for your patients and your community.
In his scholarly book, Antifragile: Things That Gain from Disorder, Nassim Taleb asserts that resilience is not enough but that we need to grow from doing hard things and become what he calls “antifragile.” It’s the idea of “posttraumatic growth.” In living organisms, it is called hormesis (small incremental stressors make an organism stronger).
He writes,
“Much of our modern, structured, world has been harming us with top-down policies and contraptions (dubbed “Soviet-Harvard delusions” in the book) which do precisely this: an insult to the antifragility of systems. This is the tragedy of modernity: as with neurotically overprotective parents, those trying to help are often hurting us the most. If about everything top-down fragilizes and blocks antifragility and growth, everything bottom-up thrives under the right amount of stress and disorder.”
Nassim Nicholas Taleb, Antifragile
Other authors and researchers have similarly been documenting societal trends toward fragility:
Michael Easter in The Comfort Crisis
Jonathan Haidt in The Coddling of the American Mind and just released The Anxious Generation
Abigal Shrier in Bad Therapy: Why the Kids Aren’t Growing Up
Jean Twenge in Generations
Today’s hyper-individualism will not easily morph into a healthy interdependence and the higher civic good. Unfortunately, polarization and tribalism based on religion, gender, or skin colour, has worsened our corporate stress levels and fragility. When we hear the line, “our community,” it often refers to a subset rather than our actual geographic village or town.
Teaching children to become healthy interdependent, selfless adults, must start in the family and parenting. Then schools and educators, faith communities, and invested non-profits must fashion curricula and training to counter today’s “sibling society.”
I have written before about the need for roundtables to explore these ideas and offer real-life advice to leaders and parents to ensure a more robust and antifragile healthcare workforce in future generations. Jonathan Haidt in The Anxious Generation offers very practical advice on ways our children might be raised in the presence of social medial, smartphones, and AI.
Cartesian dualism
René Descartes (1596–1650) taught that the mind and body were separate. While he was ahead of his time in the 1600s, he wasn’t entirely correct. In his book, Descartes’ Error, neuroscientist Antonio Damasio showed that Descartes missed both the role of emotions, and the unity of mind and body. To highlight the error, Damasio writes,
“This [correction] is anchored in the following statements: (1) The human brain and the rest of the body constitute an indissociable organism, integrated by means of mutually interactive biochemical and neural regulatory circuits (including endocrine, immune, and autonomic neural components); (2) The organism interacts with the environment as an ensemble: the interaction is neither of the body alone nor of the brain alone; (3) The physiological operations that we call mind are derived from the structural and functional ensemble rather than from the brain alone: mental phenomena can be fully understood only in the context of an organism’s interacting in an environment.”
Antonio Damasio, Descartes’ Error
Unfortunately, much of Western medicine continues in a biomedical model that we built on Descartes’ debunked dualistic theory. This results in a fix-it after its broke approach rather than upstream preventative strategies that include psychosocial (emotional) risk factors, which we now know play a huge role in adult health and chronic disease. The famous ACE (Adverse Childhood Experiences) study has definitively shown this.
A 2015 paper, Somatoform Disorders and Medically Unexplained Symptoms in Primary Care, showed that over half of presentations to primary care have psychosocial stressors as the root etiology. My fellow retired family physician colleague, Dr. Peter MacKean, has written how family doctors require more training in psychosocial diagnosing and interventions then currently offered in medical school and family medicine residency.
Many other physician writers write of this lack in physician training:
Dr. Gabor Maté in The Myth of Normal
Dr. Nadine Burke Harris in The Deepest Well
Dr. Peter Attia in Outlive
In my own work in Occupational Medicine at the Workers Compensation Board, I saw firsthand how psychosocial factors play a huge role in the outcome of workplace injuries. In some cases, it proved to be the difference between permanent impairment and worklessness versus excellent recovery and successful return to gainful employment.
As frontline clinicians in primary care, both family physicians and nurse practitioners (and other allied health workers), gain a deeper appreciation for a trauma-informed bio-psycho-social approach to prevention, investigation, and management of disease, good research predicts that outcomes and population health will improve.
Conclusion
Everyone is agreed that an efficient primary care system is the bedrock for a great healthcare system and can help mitigate heavy reliance on specialists, intensive and expensive treatments, and poor access to urgent care.
Strategies for long-term solutions will be difficult to agree on by key leaders in politics, healthcare, and educators (including healthcare worker education). The place to begin is with active listening and unselfish dialogue.
The author, Dr. Sanfilippo, a professor of medicine at Queen’s University, paints a bleak picture with around 6 million Canadians (15% of the population) without a family physician.
That made me think, “How did a G7 nation come to share the health challenges of low and middle-income countries?”
In this post I want to add some reflections on the reasons why so many Canadians do not have a family doctor. More specifically, why are young medical graduates not choosing a residency in Family Medicine and choosing other career paths.
Some history
From the dawn of Medicare in the early 1960s, to the early 1990s, was what I refer to as the “golden era” of family medicine. Prior to 1960, family doctors had significant accounts receivable from patients and families unable to pay their medical bills, and often worked pro bono. Suddenly, under Medicare, they were getting paid for their work, albeit at rates per service below other professionals such as dentists or lawyers, or colleagues south of the Canadian border. Their large practises and high throughput gave them a decent and satisfying living.
In the early 1990s, both the federal and provincial governments began to recognise that the healthcare cost trajectory under Medicare would likely be unsustainable. There was talk of too many doctors and nurses. Medical school enrollments were reduced. Recently graduating nurses couldn’t find work in Canada and were recruited to the United States (I have family members who moved to the US as nurses, married and settled permanently there).
But in my opinion, a very significant reason that family medicine lost its appeal is that the official Canadian solution to rising healthcare costs was to ration access and create gatekeepers.
Unfortunately, those gatekeepers were mostly family physicians. Here on PEI this began the much hated and maligned “complement system.”
From PEI Master Agreement ~ 1993
Here family physicians especially lost agency and intrinsic motivation, both well documented in the literature to be essential in self-determination theory and well-being. This, along with relatively poor pay under the fee-for-service system further alienated young graduates. Under fee-for-service, the emphasis became volume (10 minute consultations or less), rather than quality. Young doctors wanted a better “work/life balance,” as it became known. The larger practises of retiring physicians were unmanageable for younger successors leaving patients without the access they were used to. Doctors began to burn out under this load, only to become exacerbated during the Covid-19 pandemic. Cultural changes in patient expectations and demands also contributed to making family medicine hard.
Many Canadian provinces began to move family doctors to a salaried model, like the civil service. Here throughput became a problem, and some jurisdictions, including PEI incentivised extra work. However, decreased patient access and reduced practise sizes (panel size), began the unaffiliated (also known as orphan) patient problem noted in the Globe and Mail piece (15% of Canadians or 6 million). This was exacerbated by a growing population of immigrants and the increased needs of the elderly.
Some jurisdictions began to experiment with multidisciplinary health centres which the College of Family Physicians calls “Medical Homes.” These included nurse practitioners as well as other allied health professions working in collaboration under one roof. Initial success was reported in Ontario, but their roll-out there was halted as they were deemed too costly.
Here on PEI this is now the model going forward. I have always applauded and supported this model. I worked with non-physician primary healthcare workers and midwives in Africa and we were able to serve a population of 2 million in a hospital roughly the size of the Queen Elizabeth Hospital with around 8 physicians (albeit with much more limited resources and infrastructure). But lessons can be learned here as a rich country since we now also have limited (human) resources.
“We cannot keep doing what we have always done and expect different results.” (Some say this is the definition of insanity).
“The whole world is short-staffed.” Depending on other nations for recruitment will ultimately be futile as everyone is vying for the same nurses and doctors. And in my opinion, for a rich country to poach healthcare staff from poorer countries is less than moral or ethical.
Unity in community
We must begin with the recognition that we are ALL owners of our publicly funded healthcare system. There are longstanding “US versus THEM” dysfunctions in our system very vividly highlighted in recent media reports and townhall meetings. And a prior resignation of the entire Health PEI Board.
A “Truth and Reconciliation” moment similar to those with the injustice that our first nations endured should be undertaken in regard to the decision in Canada to ration healthcare over the backs of primary care gatekeepers. In my opinion, this is akin to abuse. This may sound strong but I practised on PEI in the 1990s and we were never officially mandated to be gatekeepers–it was subtle and under the radar.
Then, I believe we need to draw together in roundtable multidisciplinary forums to brainstorm out of the box solutions. No idea or solution should be immediately discarded as far-out. A great example for this is work by Peter Block in Community: The structure of belonging. No podium or platform or high-powered consultant to tell us how to do it. Smart people from differing disciplines sitting down in circles to build on our strengths rather than focussing on problems.
Train for real needs – and don’t burn them out before they launch
Much training is currently either wasteful or not helpful for the real needs. A four-year undergraduate degree for Medical School is unnecessary (in the UK Medical School starts after high school). I have been promoting a “gap year” doing something hard (for example, either in the Canadian north or internationally) which in my opinion (and that of other experts) would create far more people skills (EQ) and resilience than an undergraduate liberal arts or science degree.
Similarly, training RNs to be bedside nurses first and then partly through their career to train them as NPs is not in my opinion efficient. This is also problematic because we are depending on a short pool of good bedside (ER and ICU) nurses to bring them into primary care. The expertise for these disciplines is vastly different. I have written about an alternative credentialling stream (see my white paper) that could begin to produce excellently trained primary care workers for medical homes in TWO YEARS from now.
Many employers from differing industries have told me that our primary and secondary education system is not effectively training our young people for the real world of work. Parents and educators must be part of long-term discussions and solutions to prepare young people for tomorrow’s healthcare careers.
Transformational leadership
The recent crisis in the Prince County Hospital was precipitated by what leadership experts call “transactional leadership.” This is an older hierarchal leadership style hearkening back to the industrial revolution. It is a “Do as I say,” model.
Leadership experts in most every industry now agree that a Transformation Leadership style is needed in today’s world of work, especially with younger workers. I have written about the difference here.
I have worked as an occupational medicine physician for the last five years of my career and have seen the difference great bosses make in their workers throughput and resilience. This is well documented in the occupational literature (particularly Gallup data).
A famous quote by Simon Sinek is in order here:
“Leadership is not about being in charge. Leadership is taking care of those in your charge.”
Simon Sinek
Measure to find the “pinch points”
The late legendary leadership and management expert Peter Drucker said, “If you can’t measure it, you can’t manage it.”
Some things to measure (to better manage):
Wait times for an urgent appointment
How long does it take to get a receptionist on the phone?
How many ER visits are unnecessary if access for primary care was ideal?
How many patients an hour are clinicians seeing? Expected to see?
How effectively are incoming calls for appointments triaged for urgency?
A group of retired physicians, including family physicians, have authored a proposed workflow template that we believe would help Medical Homes become efficient with excellent outcomes and patient satisfaction. Click here to download and read it.
Upstream prevention
The entire theme of this website is finding “upstream solutions,” with more effective prevention strategies for many chronic diseases we now know have a singular root—systemic chronic inflammation.
Yes, we will need rescue gear and lifeboats, but a safety net above the falls would keep us all less busy rescuing people. Here is another advocacy group with similar thinking.
Psychosocial stressors and life trauma are now known to signficantly affect both childhood and adult health. Research has shown that at least 50% or more of presentations of patients for primary care are for issues related to these factors. Loneliness has also been identifiied as a large factor. There is a place for charitable, community, and faith based institutions to fill some of these needs, alleviating pressure on the biomedical healthcare community. (see work done by James Maskell at HealCommunity).
In summary
“None of us are smarter than all of us.”
Ken Blanchard
Let’s begin by creating circles of connection. Indiginous populations everywhere have always problem solved in circles. We can too. The stage and the podium were Greek inventions.
We need to train for real needs, beginning with parenthood and kindergarten, then schools, colleges, and universities. Put daily Phys Ed into every level from kindergarten to Grade 12.
Become a transformational leader and love your people like family.
Measure and identify “pinch points” in order to widen them and “relieve the pressure.”
Teach lifestyle choices to deal with the new enemy known as sugar, and its effects on insulin resistance and systemic chronic inflammation.
And finally, we need to be prepared to learn from other jurisdictions and countries rather than always needing to “re-invent the wheel.” I wrote about that in the previous post on the Times Report from the UK.
I completely agree with Dr. Sanfilippo in his Globe and Mail article:
The family physician shortage has multiple causes beyond the training process. Expectations, practice settings and compensation models are all contributing to the issue and require similarly thoughtful and disruptive innovation. We should not be passing the problem along to elected municipal officials. The time has arrived for a high-level approach involving all participants in the training continuum, focused on the current and future needs of the Canadian public. They deserve much better.
Dr. Anthony Sanfilippo, Queen University
I welcome feedback and dialogue to flesh out these ideas. These views are my opinions based on my own experiences practising here on PEI as a family physician for 32 years, as an occupational medicine physician with the Workers Compensation Board for 5 years, and in my early career for 5 years in West Africa, and subsequently leading small capacity building medical teams to East Africa as well.
The problems facing the the NHS (National Health Service) in the UK are pretty similar to ours in Canada — family physicians leaving practises, long surgical wait times, poor access to primary care, backed up ambulances at the ER (emergency rooms or A&E’s as they call them).
The Times and Sunday Times (of London) established a Health Commission a year ago to investigate and make recommendations on England’s health and social care crisis. Their report and 10 recommendations have just been made public (Feb 5, 2024).
It has always been my belief that “all of us are smarter than some of us,” and that we can learn valuable lessons from other nations — both rich and resource challenged ones.
The UK report has valuable evidence based findings and its authorship was truly multidisciplinary with expertese from many fields. Here in Canada (and here I am also thinking of my home province of PEI), we need similar multidisciplanry dialogues. And those dialogues can utilize much of the work and research already done by think tanks such as the Times Health Commission and institutions like the Fraser Institute.
Here are the main 10 recommendations (some of which are applicable here):
Create digital health accounts for patients, called patient passports, accessed through the NHS app to book appointments, order prescriptions, view records, test results or referral letters and contact clinicians.
Tackle waiting lists by introducing a national programme of weekend High-Intensity Theatre (HIT) lists once a month in 50 hospitals to get through a week’s worth of planned operations in a day and create seven-day surgical hubs.
Reform the GP contract to focus on wider health outcomes rather than box-ticking, ensure patients get prompt appointments and restore continuity of care. Encourage more super-practices and create community health centres.
Write off student loans for doctors, nurses and midwives who stay in the NHS to improve retention as well as recruitment. Debt should be cut by 30 per cent for those who stay three years, 70 per cent for seven years and 100 per cent for ten years.
Introduce no-blame compensation for medical errors with settlements determined according to need to ensure families get quick support and encourage the NHS to learn from mistakes.
Establish a National Care System giving everyone the right to appropriate support in a timely fashion. Equal but different from the NHS, it should be administered locally and delivered by a mixture of the public and private sectors.
Guarantee that all children and young people requiring mental health support can get access to treatment within four weeks and rapid follow-up appointments. Publish data on waiting times for all mental health services.
Tackle obesity by expanding the sugar tax, taxing salt, implementing a pre-watershed ban on junk food advertising and reducing cartoons on packaging to minimise children’s exposure to unhealthy food.
Incentivise NHS staff to take part in research, and put the case for research to their patients by giving 20 per cent of hospital consultants and other senior clinicians 20 per cent protected time for research.
Establish a Healthy Lives Committee empowered by a legally binding commitment to increase healthy life expectancy by five years in a decade and reduce health inequalities to encourage a long-term approach with cross-party agreement.
PEI health reform progress
We are already tackling several of these (similar) recommendations here and I am grateful for leaders who have a vision for sustainable and equitable healthcare for all.
# 1 is well underway with the Electronic Medical Record (EMR) rollout (all functionality is still pending). Our version of # 3 is also underway with current negotiations for a new contract for PEI Medical Society physicians (hopefully with an emphasis on primary care). Youth mental health services are also recognized as a significant area of need.
#’s 8 and # 10 are under the leadership of the Deputy Chief Public Health Officer. A Live Well PEI website is active. I have been told that there are plans to share a provincial wellness action plan in 2024. I have written about # 8 here.
Reports of progress in the rolling out of Patient Medical Homes are positive although the patient registry has not reduced.
Further PEI dialogue is needed
Recent crises in PEI’s second largest hospital have led to public debate with politcal and healthcare leaders. While this crisis must be resolved, it really only represents an iceberg tip of deeper unsustainable problems.
I encourage wider multidisciplinary rounttable discussions to build on reform advances, lessons from other nations, and our own unique “out of the box” thinking. We must address the US versus THEM criticisms highlighted in recent publicized comments from former leaders.
Having served as an occupational medicine physician, I have firsthand knowledge that healthy workplaces (all sectors, but especially health) are essential. Workforce resilience needs to be addressed beginning in childhood with parenting and educational strategies.
I have previously written my opinion on efficient use of non-physician primary health clincians (mostly NPs here, but includes PAs (physician assistants), pharmacists, and now also midwives). The gap left by exiting family physicians needs a sustainable long-term solution.
Please don’t hesitate to contact me if you would like to participate in further dialogue.
According to Diabetes Canada, one third (33%) of Canadians will likely have either diabetes or one of its forerunners by 2032. The downstream healthcare burden and costs, on top of the stretched Canadian healthcare system, are staggering. Diabetes, and its related metabolic disorders, contribute to 30% of strokes, are the leading cause of blindness, cause 40% of heart attacks, 50% of kidney failure requiring dialysis, and 70% of leg and foot amputations. It’s an escalating global problem according to both the WHO (World Health Organization) and the IDF (International Diabetes Federation).
This post will highlight causes for this rising health crisis and offer solutions which all citizens need to take responsibility for. The focus will be on Type 2 Diabetes (Type 1 diabetes usually starts in early life and has a very different cause than the more common Type 2 variety), and its frequent forerunner, metabolic syndrome.
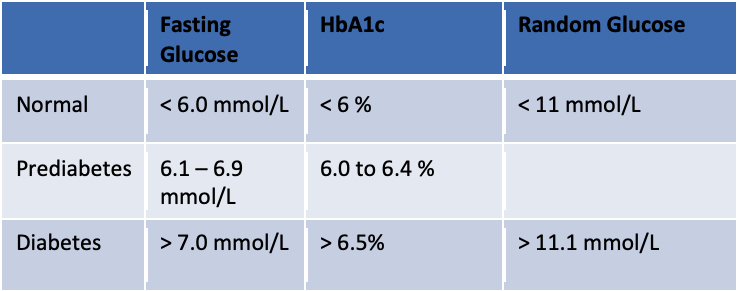
How we diagnose diabetes and prediabetes
Table 1 below shows the simple blood tests used to diagnose diabetes. Glucose is one of the two molecules in sucrose (common sugar), the other being fructose. A fasting glucose is a blood test that measures the blood sugar circulating in the bloodstream after a typical overnight fast. A random glucose is taken regardless of fasting state. The HbA1c refers to glycosylated hemoglobin. This is the per cent of hemoglobin (in red blood cells and which carries oxygen) that has a glucose molecule attached to it. The longer the hemoglobin is exposed to elevated blood glucose levels, the larger the per cent of hemoglobin that becomes glycosylated (or “sweetened”) by a glucose molecule. This is a good measure of average blood sugars over the recent three months.
Table 1 – How to diagnose diabetes in Canada
There is another blood test which can detect earlier signs of prediabetes before the fasting glucose begins to rise. Insulin levels can be measured to detect hyperinsulinemia, but this is not a standard test and rarely used by most doctors or nurse practitioners. Insulin becomes elevated because there is resistance to it by muscle cells and fat cells, requiring ever increasing amounts to keep the blood sugar normal. This insulin resistance is a major factor leading to full blown diabetes and all its end organ damaging effects. And it is almost always present in what we now call metabolic syndrome.
What is metabolic syndrome?
Metabolism is the way our body converts the energy in our food, into the energy needed by our cells (such as brain cells and muscle cells), to do their job (cognition or movement). The term metabolic dysfunction simply refers to something awry in the pathway between food energy to cell energy (mostly ATP or adenosine triphosphate). Diabetes, prediabetes, and hyperinsulinemia are all evidence of metabolic dysfunction.
Metabolic syndrome is now known as a specific condition that can be diagnosed by the presence of 3 (or more) out of the following 5 conditions:
High blood pressure (essentialhypertension)
High triglycerides (on a fasting blood test)
Low HDL cholesterol (also on a fasting blood test)
Large waistline (waist > 40” (94 cm) in men, 35” (82 cm) in women)
Elevated fasting glucose (> 6.0 mmol/L)
While not required for a diagnosis, polycystic ovarian syndrome (PCOS) is also often associated with metabolic syndrome in women. About 40% of adult woment and nearly 1/3 of adolescents with PCOS have metabolic sydrome.
It is estimated that in North America, 1 in 3 adults have metabolic syndrome. Some estimates are even higher, given the rising rates of obesity here.
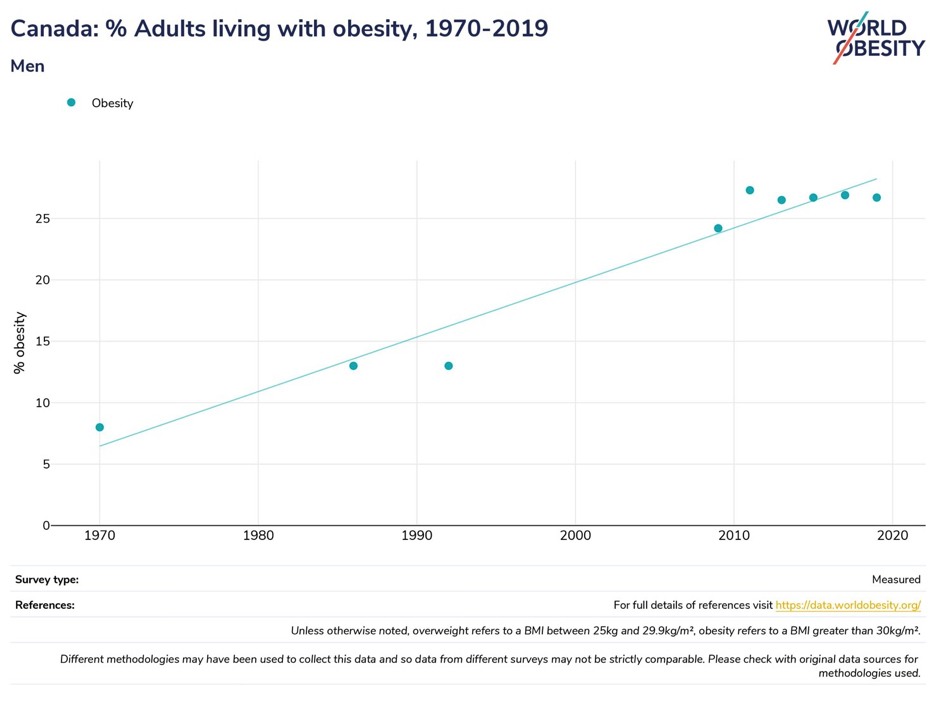
Obesity rates in Canada
The Figure 1 chart below documents the rising rates of obesity in Canada between 1970 and 2019. The definition for obesity here is a BMI (body mass index) of 30 kg/m2 or more.
Figure 1 – Canadian Obesity Rates
This shows prevalence rates of obesity over 25%. But even more significant, is that when overweight Canadians are added (BMIs between 25 and 29.9 kg/m2), the rates jump to over 60%.
Being overweight or obese is a major risk factor for insulin resistance and its downstream effects on both physical and mental health.
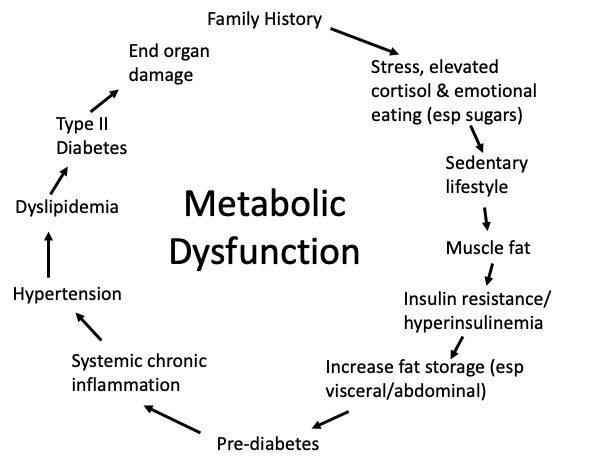
The metabolic dysfunction pathway
Figure 2 is a typical pathway that leads to ill-health on multiple fronts. It’s also a cycle because there is a tendency to perpetuate itself after end organ damage begins; stress invariably increases, as does emotional eating and a sedentary lifestyle.
Figure 2 – The Metabolic Dysfunction Cycle
Type 2 diabetics often have a family history for diabetes. There are also ethnic differences, with some increased risk among First Nations adults, as well as South Asians, for example. With recent understanding of epigenetics, it is unclear how much of inherited diabetes is genetic (nature), versus epigenetic (nurture). Which leads to step 2 of our cycle—stress.
Prenatal and childhood stressors (known as ACEs, for adverse childhood experiences) predispose a child (and the later adult) to hyper-vigilance, and elevated levels of the stress hormone cortisol. This is part of the “fight or flight” hormonal system designed for our protection from danger. One of the functions of cortisol as a stress hormone is to ensure adequate blood sugar levels for fighting or escaping. And, with prolonged stress, and prolonged elevated cortisol levels, appetite is likely to increase, with sugar craving. This may start a long road beginning with childhood obesity.
Emotional overeating often co-exists with a sedentary lifestyle. It is now thought that the first step toward insulin resistance is fat deposition into muscles (like marbled steak). Clearly, excess carbohydrates and inactive, flabby muscles, play a role.
With elevated insulin levels that to this point can keep blood sugars (and tests) in normal ranges, something sinister happens in the abdominal cavity in particular. One of the functions of insulin is to push excess calorie energy into storage, either in the liver as glycogen, but also into fat cells. The fat cells in the abdomen, including organs like the liver and the pancreas, and in the omentum (a fatty apron-like layer over the intestines) begin to swell with fat. This often leads to non-alcoholic fatty liver disease (NAFLD) and fatty pancreas. This is where the abdominal girth measurement noted above as a finding in metabolic syndrome is relevant. You may have read of the “apple” shaped body habitus versus the “pear” shape. It is the apple that may be a problem. There are other fancy tests that some private clinics recommend measuring abdominal (also known as visceral) fat. Here in our health system, an abdominal ultrasound will often reveal a fatty liver. And a fatty pancreas, where insulin is produced, may begin to slow insulin production.
By this point on our cycle, it is likely possible to find evidence for prediabetes on careful testing (either a glucose tolerance test or a fasting insulin level). But what is most disturbing at this point toward a healthy lifespan (so-called “healthspan”) is systemic chronic inflammation. And this has a lot to do with two factors: 1) chronically elevated cortisol levels and 2) abdominal fat cells that leak proinflammatory cytokines (these are substances that cause low-grade or frank inflammation).
Both chronically elevated cortisol levels and systemic chronic inflammation affect brain and nervous tissue health. This is called neuroinflammation, and now understood to be a significant contributor to mental illness (such as depression and bipolar illness and the neurodegenerative disorders (such as dementia). This is also likely a significant factor in lingering symptoms after a (sometimes minor, or repeat) concussion.
Chronic stress, elevated cortisol, and chronic inflammation all contribute to many of the chronic diseases taking up so much of our healthcare resources: cancer, strokes, heart disease, chronic pain, autoimmune disorders, etc.
Once the cycle reaches the top again, lifestyle patterns, stress, and genetic material, all get passed to the next generation, and the transgenerational cycle begins again.
How do we interrupt the cycle?
Clearly, the earlier we can intervene in the cycle, the better outcomes we can expect both individually, in families, and in the community. Family and relational health that can welcome a newborn into a stable, loving environment is key. Then physical activity and a healthy diet of whole foods away from excess sugars and carbs, in particular ultra-processed foods, are essential for all. And meaning and purpose, contribution, and community, rather than the “me” of individualism. Healthcare professionals need to be trauma-aware and able to address psychosocial factors early, long before downstream disease takes hold.
I support the Live Well PEI initiative. Let’s get the message out.
I also believe we need to convene roundtable discussions with key stakeholders from disciplines including healthcare, education, the faith community, charities, politics, sports and fitness leaders, business leaders, and parents to explore the cultural transformation changes needed to ensure resilient and thriving families and workforce.
This is no easy task. But I for one, believe that none of us is as smart as all of us. There are, for example, lessons to be learned from educational and parenting styles from other countries (look at Finland’s educational success, for example).
I am encouraged by the collaborative practice model being rolled out (Patient Medical Homes) on PEI. But to be successful, we as citizens we must ALL do our part as we are all OWNERS of our publically funded healthcare system—for the sake of our elders and future generations.
If you would like to be part of roundtable discussions, please contact me, or the Live Well Health Promotion Team at livewellpei@ihis.org
My team and I also offer a 10 hour Well-Being Masterclass that can be offered in a weekend retreat setting or over 5 evenings. We cover all four quadrants of a healthy and thriving lifestyle: Physical disciplines, Mental health and character, Spiritual meaning and purpose, and Relational belonging nad connectedness. Contact me for more information or to request the course.
This is the inspiration to the theme of “Upstream Well-Being Solutions.” My wife and I recently completed a long road-trip covering 26 states in America. Waterfalls were a common theme, as was rivers (we crossed the Mississippi twice, walked along the Rio Grande, and picnicked on the Colorado.
Here we are at Twin Falls (the “Niagara of the West”) in Idaho. These falls are on the Snake River.
It struck me that so much of our health system and the way we live our lives are focussed on radical interventions after we have a healthcare crisis, or a personal health crisis.
Let’s begin to think about ways to intervene above the falls before drifting over the falls.